Katharina Schroth’s Scoliosis Treatment Method
Katharina Schroth was born February 22, 1894, in Dresden, Germany. She suffered from moderate scoliosis and underwent treatment with a steel brace at the age of sixteen before she decided to develop a more functional treatment approach. Inspired by a balloon, she tried to breathe away the deformities of her own trunk by inflating the concavities of her body selectively in front of a mirror. She also tried to “mirror” the deformity by overcorrecting with the help of certain pattern specific corrective movements. She recognized that postural control can only be achieved by changing postural perception.
This new treatment concept consisting of specific postural correction, correction of breathing patterns, and correction of postural perception was introduced at a small institute she had established in Meissen, Germany, with rehabilitation taking place over the course of three months. Beginning in the late 30s and early 40s, she was assisted by her daughter, Christa Schroth, a collaboration that spanned decades. It wasn’t until the late 1980s that the first studies of Schroth methodology were carried out. The patient series for the first prospective controlled trial was derived from the patient samples of 1989-1991.
Over time, the content has evolved and rehabilitation times have changed. Bracing has been introduced and refined for Schroth compatibility to offer patients improved treatment outcomes. In the last few years, the first author modified the older techniques thereby modernizing the program and reducing training times by adding new forms of postural education such as sagittal correction, activities of daily living (ADL) correction and experiential learning.
Schroth Program
While the program is still based on the original approaches of the three-dimensional treatment according to Katharina Schroth – specific postural correction, correction of breathing patterns, and correction of postural perception – the patient is now instructed in a way where these concepts can more easily be applied during daily routines.
The Schroth Method and Its Evolution
The history of conservative treatment of scoliosis is rather long and leads us back to the original methods of Hippocrates, 460-370 BC (Vasiliades et al. 2009). Although more than 2000 years have passed since the days of Hippocrates, the main approach of conservative scoliosis treatment in the early 20th century was still based on mechanical viewpoints or concepts related to approaches still used today.
Correction exercises were used widely throughout Europe during the last two centuries. Some of them requiring three therapists for one patient during scoliosis correction (Oldevig 1913). The history of the Schroth method involves the professional work of three generations. The initiation of the program was the result of Katharina Schroth’s self-study, in part as a result of analyzing her own body, her own spinal function, and the corrective movement patterns.
Mirror monitoring took on an important role in the original Schroth program, as it does in current protocols, and allows the patient to synchronize the corrective movement and postural perception with visual feedback. Since breathing and its functional correction play such a key role, her first writings focused on breathing in general. Later, she also described the importance of postural perception by the patient and its improvement via specific correction exercises.
Recent Developments
With far more than 50,000 evaluations of in-brace x-rays over the past thirty years, the first author has continuously improved not only in-brace corrections, but also the effectiveness of the corrective movements. Since the 2006 add-ons, training times have been shortened, but the concepts are still based on the original three-dimensional treatment approach according to Katharina Schroth.
In 2010, the Schroth Best Practice program was officially established. Patients can achieve results within a week, or less, which rivals the previous four to six weeks of inpatient rehabilitation. Meanwhile, Scoliosis Short-Term Rehabilitation (SSTR) has been tested and the results, as achieved in the pilot investigation, have been shown to be repeatable worldwide.
Physical rehabilitation which focuses on ADLs to avoid loss of postural control during everyday activities is advisable. Add-ons derived from the original Schroth approach aim at unloading the curve and are essential elements for postural control. It is important to note that thirty minutes of scoliosis exercise daily is less effective without knowledge of curve-pattern specific ADLs since without them the curve(s) are loaded during the rest of the day. It should also be noted that it is important to incorporate physical rehabilitation during brace wear whenever possible, with more intensive work as the patient is weaned from the brace.
The newest evolution of Schroth-based therapy is preferred in curves less than 70° because it is simpler for the patient, addresses the sagittal plane, makes the patient aware of the importance of unloading the spine, and emphasizes the maintenance of postural corrections whenever possible throughout the course of the day.
The development of three-dimensional scoliosis treatment according to Schroth has taken place in three steps since its origin 100 years ago.
1. The program originally developed by Katharina Schroth – the original – was in principle a program focused on a single curvature pattern for thoracic major curvatures with individual modifications. The sagittal correction principles were lumbar delordotic and thoracic anticyphotic. After all, this is the only way to correct the protruding rib hump in such large thoracic scolioses.
2. The further development of Christa Lehnert-Schroth took into account the fact that Katharina Schroth’s original program was not applicable to lumbar curvatures. She therefore developed her own series of exercises for patients with lumbar and thoracolumbar curves and a small but meaningful classification (functional 3-curve / functional 4-curve). Retrospectively, we now call this program, which is geared to two different curvature patterns, the intermediate Schroth program, which continues today largely unchanged in the Bad Sobernheim School and the Barcelona School. Only the terminology has changed from the time.
3. The Schroth Best Practice Program, or SBP for short, is characterized by a system of treatment modules which, in a logical sequence, take into account all aspects of specific scoliosis treatment known today.
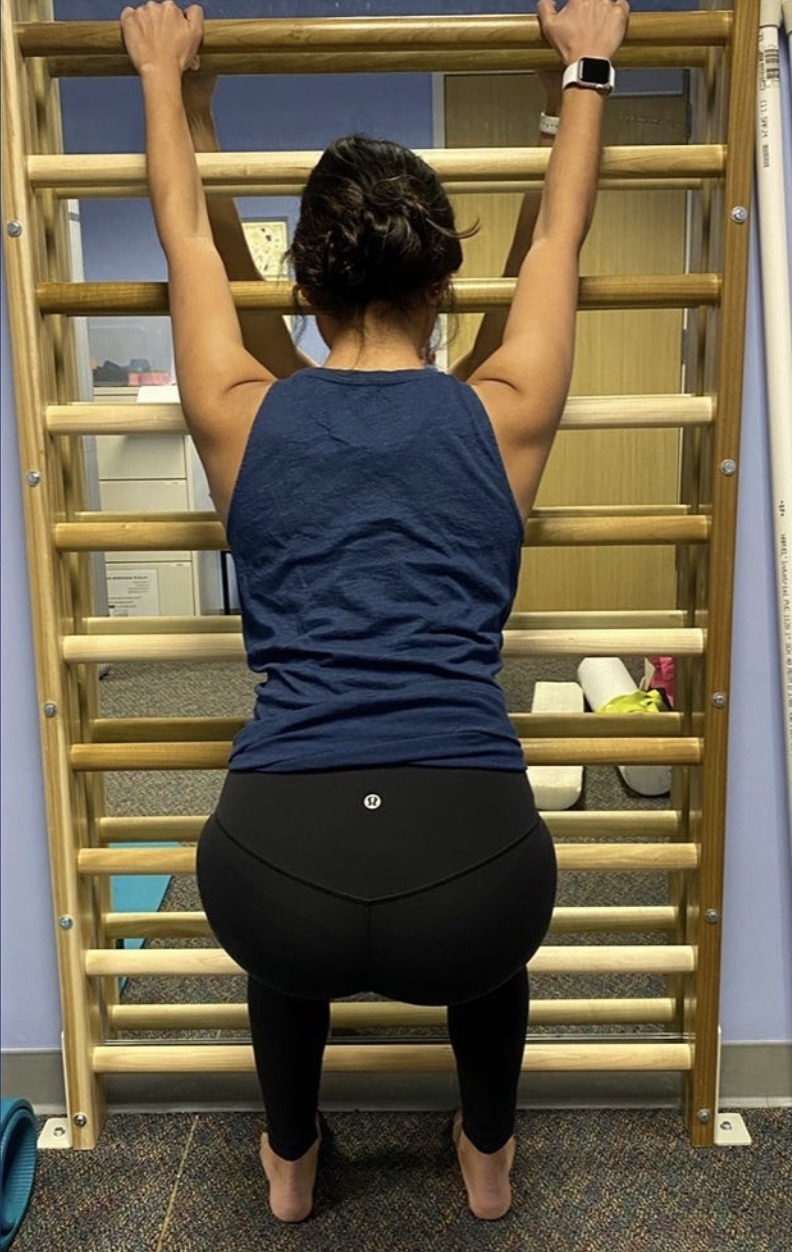
Schroth Exercises for Scoliosis
Can Reverse Curvature Quickly and Safely — Without Surgery
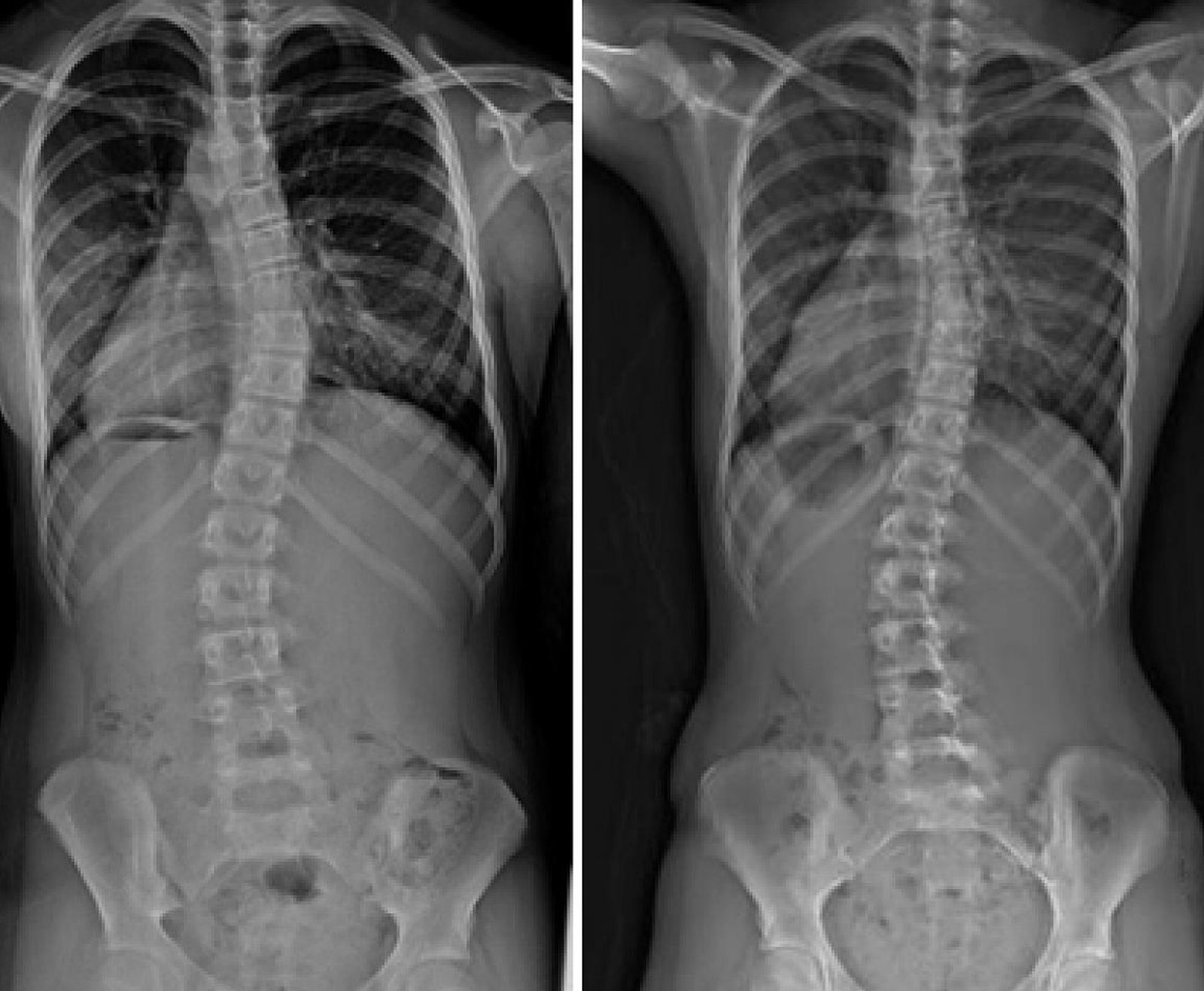
schroth-method-boy-before-and-after
5-year-old boy, scoliosis resulting from polio (First).
After 3 weeks of intensive Schroth treatment (Second).
After 8 weeks of Schroth scoliosis exercise therapy (Third).
How the Schroth Method Works
Elongate and Derotate Your Spine
Schroth Exercises Are Customized for Your Unique Spinal Deformation.
The method teaches you how to:
⦁ Correct spinal rotation and increase lung capacity with a rotational breathing technique.
⦁ Help restore normal spinal position with pelvic corrections, breathing technique, and stabilizing isometric contractions.
⦁ Improve your posture during routine daily living, not just during therapy.

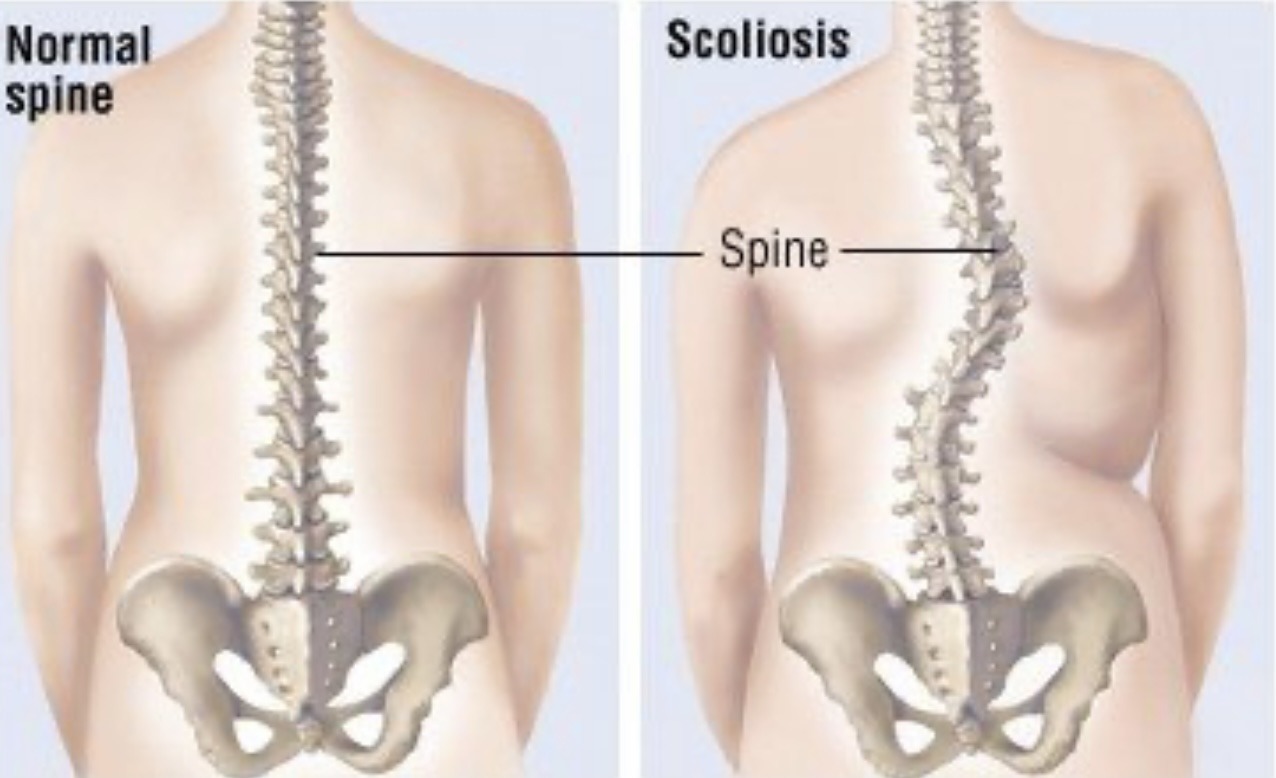
Scoliotic Imbalances and Rotations
For at least fifty years, clinical studies of scoliosis frequently have reported paraspinal muscle imbalances of strength, diameter, length, fiber type, or electromyographic activity. They support the Schroth thesis that scoliosis always involves asymmetrical muscle groups in the back and elsewhere, which in normal bodies are more evenly symmetrical.
In a typical scoliotic configuration, depicted at right, back musculature pulls lower ribs so that the lumbar (abdominal) region rotates laterally, downwards, and backwards.
To maintain the torso’s upright and forward orientation, the thoracic (chest) region must twist back in the opposite directions, and the cervical (neck) area responds with a third abnormal twist. Other imbalances are often present in the legs and feet. The resulting eccentric loads predispose the scoliosis to a vicious cycle of progression with unpredictable outcome.
In its effort to reverse the scoliotic spinal rotations, the Schroth method of scoliosis exercise therapy addresses all three planes — sagittal, frontal, and transverse. This means that correction needs to occur not only from side to side and front to back, but also longitudinally: that is, the spine which has shortened because of rotation must also be lengthened. Hence the Schroth method’s designation as “three-dimensional” therapy.
Schroth Treatment Goals
The scoliosis exercises are designed to reverse all of the abnormal curvatures with a variety of means, based upon the therapist’s analysis of a patient’s muscle imbalances. Christa Lehnert-Schroth writes in her book:
Scoliosis is characterised by a more or less pronounced change in the balance of forces, starting already in the feet, legs and hips, with inequality of muscles in terms of length and size. The greater the deviations from the midline, the longer the affected muscles become and the more volume is lost. They become flaccid and finally inactive. They lose their supportive function. Shape changes are only possible because the muscles permit them to happen. They become longer or shorter depending on the direction in which the trunk is moved and rotated. In other words, deviations of the trunk to the side or backwards can only develop if the corresponding supportive muscles give way and become elongated.
Therefore, treatment must improve posture so that the body can regain its original vertical axis. This can only happen by developing and training the corresponding muscle groups responsible for upright posture. To restore muscular balance, those muscles that have grown longer must be shortened and those that have become shorter must be lengthened. In order for these to be able to hold the spinal column and ribcage in their normal vertical position again, they need to be strengthened — and on both sides. It is absolutely essential that the inactive, shortened muscles perform strength work in the lengthened state. [pp. 42-43]
The basis of correction is a properly aligned pelvis. A scoliotic pelvis is often not only shifted laterally but also tilted and rotated. Therefore the spine, which attaches to the pelvis via the sacrum, has a misaligned foundation. The Schroth method first addresses the patient’s pelvis position with five corrections.
The treatment can then focus on spinal elongation, and on derotation by means of individually designed scoliosis exercises.
One of the primary Schroth tools is strengthening exercises tailored to the individual patient. Another, the unique rotational breathing technique, focuses on vertebral derotation using the ribs as levers, as well as on increasing the patient’s vital capacity. Read about Exercises for Scoliosis to see a few sample Schroth method scoliosis exercises designed for a specific patient.

About Dr. Sam Dyer | Osteopath
Sam completed his studies at RMIT University, following completion, Sam moved to Queensland where he worked rurally treating a wide range of patients for the first 18 months of his career. Following his time in QLD, Sam returned to Melbourne and has been working in private practice for the last 4 years. Sam is available at both of our Bayswater North and Lilydale clinics.Sam developed his passion for Osteopathy by pursuing the holistic principles of health care that Osteopathy is founded on. Sam’s treatment is strongly guided by the idea that the body is a unit, combining hands-on treatment, dry needling, exercise and education to reach the best possible outcomes for his patients. Sam also has a passion for treating and managing patients suffering from scoliosis related pain since completing the “Schroth Best Practice” course in April of 2023.
Outside of the clinic, Sam thoroughly enjoys exploring his interest in human movement and biomechanics in both his own training and by continuing to educate himself in this area with books and podcasts. He also thoroughly enjoys being outdoors, especially anywhere you can do a bit of fishing.
